Tirzepatide vs. Semaglutide
Which Weight Loss Peptide Actually Works Better in 2026?
5/8/20248 min read

Which Weight Loss Peptide Actually Works Better in 2026?
If you've been hearing about GLP-1 weight loss drugs, the two names that come up most are tirzepatide and semaglutide. They are the most-prescribed and most-discussed peptides in 2026 — sold under brand names like Ozempic, Wegovy, Mounjaro, and Zepbound. Both are weekly injections, both can produce dramatic weight loss, and both have changed how doctors approach obesity and type 2 diabetes.
So which one actually works better? The short answer: in clinical trials, tirzepatide produced more weight loss on average than semaglutide. But that is not the whole story — the two peptides differ in how they work, what side effects they tend to produce, what they cost, and who they are best suited for.
This guide compares them across the dimensions that matter most for someone considering treatment in 2026: mechanism, real trial results, side effects, dosing, access, and cost. By the end, you'll have a clear picture of which fits which kind of patient — and the questions to bring to your doctor.
What Are Tirzepatide and Semaglutide?
Both tirzepatide and semaglutide belong to a family of peptide-based medications called incretin mimetics. They copy the action of natural gut hormones your body releases after a meal — hormones that signal fullness, slow digestion, and improve insulin response. Both are FDA-approved and prescribed for type 2 diabetes and chronic weight management.
Semaglutide: the original GLP-1 agonist
Semaglutide is the older and more familiar of the two. It was approved for type 2 diabetes in 2017 (sold as Ozempic) and for obesity in 2021 (sold as Wegovy). An oral form, Rybelsus, also exists for diabetes. Semaglutide acts on a single receptor: GLP-1, or glucagon-like peptide-1.
Tirzepatide: the dual-receptor newcomer
Tirzepatide was approved in 2022 for diabetes (Mounjaro) and in late 2023 for obesity (Zepbound). It activates two receptors at once: GLP-1 and GIP (glucose-dependent insulinotropic polypeptide). This dual-agonist design is the key structural innovation.
Both medications are weekly injections taken with prefilled pens, and both have completed major Phase 3 clinical programs. The difference between them is structural, and that difference shows up consistently in clinical results.
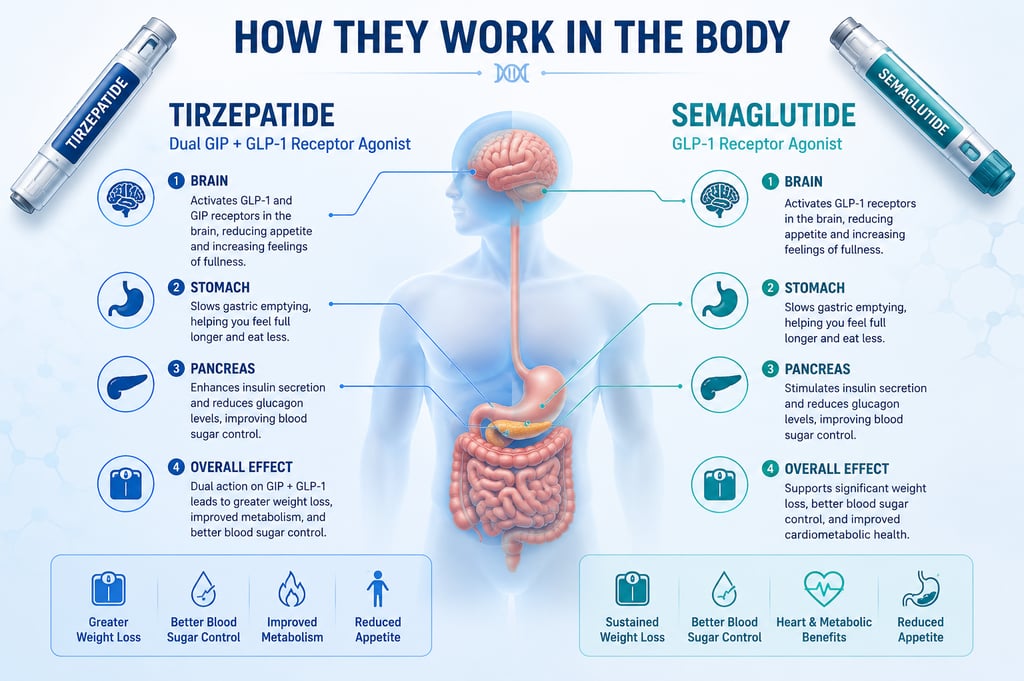
How do they work in your body?
Both peptides start the same way. After injection, they travel through the bloodstream and bind to receptors on cells in the pancreas, brain, and gut. Once bound, they trigger a cascade of effects: more insulin released when blood sugar is high, less glucagon (which raises blood sugar), slower stomach emptying, and reduced appetite signals from the brain.
Semaglutide does all of this through GLP-1 receptors alone. The molecule was engineered as a long-acting analog of natural GLP-1, with chemical modifications that prevent rapid breakdown and allow weekly dosing.
Tirzepatide adds a second mechanism. By also binding GIP receptors, it activates a separate but overlapping signaling pathway. GIP is the other major incretin hormone — released from the small intestine after eating — and it appears to amplify insulin release, modulate fat storage, and possibly enhance the body's response to GLP-1 itself.
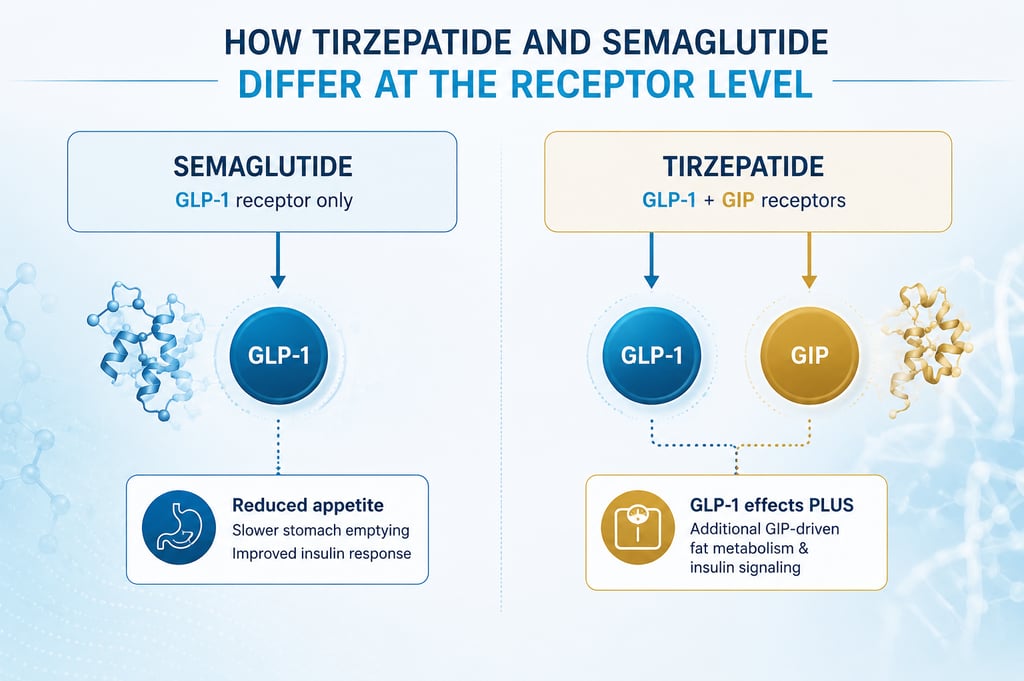
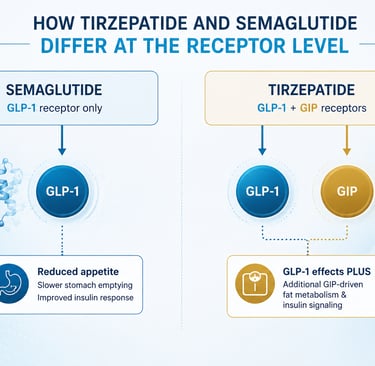
Tirzepatide hits two targets, semaglutide hits one — and that single change appears to matter for weight outcomes. Researchers still debate exactly how much of tirzepatide's edge comes from GIP signaling itself versus how the dual mechanism reshapes appetite and metabolism. According to reviews published in Nature Reviews Endocrinology, this incretin-mimicking approach is also what makes both drugs safer than older medications that forced insulin release regardless of blood sugar level.

Weight Loss Results: What the Trials Show
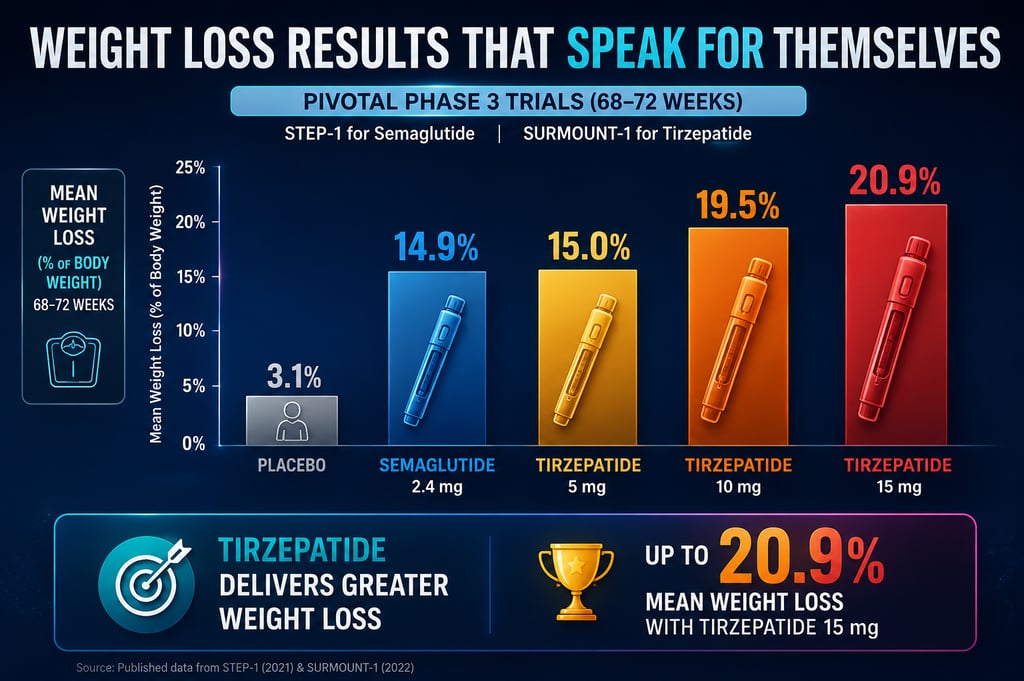
The most direct evidence comes from two large Phase 3 programs: STEP-1 for semaglutide and SURMOUNT-1 for tirzepatide. Both were placebo-controlled trials in adults with obesity, both ran for over a year, and both used lifestyle counseling alongside the medication.
In STEP-1, published in the New England Journal of Medicine in 2021, participants taking semaglutide 2.4 mg weekly lost an average of about 14.9% of their starting body weight over 68 weeks, compared to 2.4% in the placebo group. SURMOUNT-1, published in 2022, tested three doses of tirzepatide. At the highest dose (15 mg), participants lost an average of 20.9% of body weight over 72 weeks. Even the lowest tested tirzepatide dose (5 mg) produced a similar result to top-dose semaglutide.
In published Phase 3 trials, tirzepatide consistently produced greater average weight loss than semaglutide. The first head-to-head trial, SURMOUNT-5, reported in 2024 that tirzepatide produced significantly more weight loss than semaglutide in the same study population — confirming what indirect comparisons had suggested. Individual results vary widely, however, both drugs have responders who lose 25% or more, and non-responders who lose very little. The averages tell you what to expect across a large group, not what will happen to any single person.
How They're Taken in Clinical Practice
Both medications are weekly subcutaneous injections, almost always given via a prefilled pen. Most patients inject into the abdomen, thigh, or upper arm. The needles are small and the procedure takes seconds; clinicians teach self-injection in a single visit.
Dosing in published trials
Both drugs use a slow dose-escalation schedule, where the dose is increased every four weeks to limit side effects. In STEP-1, semaglutide started at 0.25 mg weekly and titrated up to 2.4 mg over 16 weeks. In SURMOUNT-1, tirzepatide also started low and was titrated to a maintenance dose of 5, 10, or 15 mg weekly depending on trial arm. These are the dosing schedules clinicians follow today.
These dosing numbers come from registered clinical trials and FDA-approved prescribing information; they are not a recommendation. Real-world prescribing varies by patient response, tolerability, and provider judgment.
What patients can expect day-to-day
Most patients describe the injection itself as quick and largely painless. Hunger reduction usually appears within days, but full appetite suppression and weight loss build over months. Both medications are weekly subcutaneous injections, almost always given via prefilled pen, which makes them easy to fit into a normal routine. If a dose is missed, both have published guidance for resuming.
Side Effects and Tolerability
Most side effects of both drugs are gastrointestinal. The most common are nausea, vomiting, diarrhea, constipation, and stomach pain. These tend to be most pronounced during dose escalation and ease as the body adjusts.
Most side effects are gastrointestinal and tend to ease over time as the dose increases gradually. For most patients, slowing down the titration is enough to manage them. A smaller share of patients stop treatment due to nausea.
Less common but more serious risks
Both drugs carry warnings for pancreatitis, gallbladder disease, and possible thyroid C-cell tumors (the latter based on rat studies; human relevance is debated). Severe gastroparesis (delayed stomach emptying) has been reported in a small number of cases. Both are contraindicated for people with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia type 2.
Side effect profiles between the two are similar in published trials, though some studies suggest tirzepatide produces slightly more nausea at higher doses. A qualified prescribing clinician will review your full medical history before deciding which drug, and which titration pace, fits you.
Cost, Insurance, and Access in 2026
List prices for both drugs hover around $1,000–$1,400 per month in the United States as of 2026, though insured patients often pay much less. Coverage varies dramatically: many commercial insurers cover both drugs for type 2 diabetes, and a growing share now cover them for obesity when specific BMI and comorbidity criteria are met.
Insurance coverage is the single largest factor that determines which drug a patient ends up on, more so than clinical preference. Some plans cover only one of the two; others require step therapy starting with semaglutide before tirzepatide is approved. Check your formulary before assuming either is available to you.
Compounded versions sold through telehealth platforms filled gaps when brand-name supply was constrained, but FDA scrutiny tightened in 2025–2026 and many compounding shortcuts are no longer allowed. Stick with FDA-approved versions when possible — purity, dose accuracy, and safety oversight are higher than what is available from research suppliers or grey-market vendors.
Manufacturer savings programs can also dramatically lower out-of-pocket cost for eligible patients. Both Eli Lilly and Novo Nordisk offer co-pay assistance and direct-to-consumer programs that have shifted real prices in 2026. A pharmacist or prescriber can help you compare what each path actually costs once savings cards are applied.
Who Should Choose Which?
The right choice depends on your goals, your tolerability, and what your insurance will pay for. Both drugs work, both are well-studied, and both are reasonable starting points.
Tirzepatide may make sense if
You have a higher target for weight loss, you have type 2 diabetes with poor glucose control, your insurance covers it on equal terms, or you've tried semaglutide without enough response. Trial data suggest a higher ceiling on weight outcomes — particularly at the 10 mg and 15 mg maintenance doses. Patients seeking to reach a specific BMI threshold or address insulin resistance often find tirzepatide produces results faster.
Semaglutide may make sense if
You have a longer track record on the drug, your insurance covers it more readily, you tolerated it well already, or your prescriber feels its longer real-world history is reassuring for your case. Semaglutide also has the most extensive cardiovascular outcomes data — the SELECT trial showed a meaningful reduction in major adverse cardiovascular events in patients with established heart disease. For patients where cardiovascular risk reduction is a co-equal goal alongside weight loss, that body of evidence still tilts the conversation toward semaglutide.
Frequently asked questions
How does your product/service work?
On average, tirzepatide produces about a third more weight loss than semaglutide in published trials, not 50%. SURMOUNT-5, the first head-to-head Phase 3 trial published in 2024, reported around 20% weight loss with tirzepatide versus 14% with semaglutide. The advantage is real but modest, and individual response varies widely.
Can you switch from semaglutide to tirzepatide?
Yes, with a clinician's guidance. Most providers stop semaglutide for a week, then start tirzepatide at the lowest dose and titrate up to limit side effects. Switching is common when weight loss has plateaued on semaglutide or when insurance changes. Never switch on your own without a prescription and supervision.
Do you regain weight if you stop?
Often, yes. Both STEP and SURMOUNT extension data show that most weight is regained within a year of stopping the drug. Researchers describe these medications as a long-term treatment for a chronic condition, not a short-term diet aid. Discuss long-term plans with your clinician before starting.
Are tirzepatide and semaglutide considered peptides or drugs?
Both. Each is a peptide — a chain of amino acids — but each has been chemically modified for stability and is regulated as a small-molecule pharmaceutical. They sit firmly inside conventional medicine, distinct from research peptides like BPC-157 that operate in regulatory grey areas.
Are compounded versions of these peptides safe?
Both. Each is a peptide — a chain of amino acids — but each has been chemically modified for stability and is regulated as a small-molecule pharmaceutical. They sit firmly inside conventional medicine, distinct from research peptides like BPC-157 that operate in regulatory grey areas.
What's coming after tirzepatide and semaglutide?
The next generation includes triple agonists like retatrutide, which targets GLP-1, GIP, and glucagon receptors. Phase 2 results showed weight loss exceeding 24% over 48 weeks. Retatrutide is currently in Phase 3 trials and could become available within the next few years if results hold up. [INTERNAL LINK: Retatrutide guide — Post 5]
The Bottom Line
Tirzepatide and semaglutide are both highly effective weight-loss medications backed by strong clinical evidence. On average, tirzepatide produces more weight loss, but semaglutide has a longer track record and broader insurance coverage in many plans. For most patients, the practical question is not which drug is theoretically better, but which one fits your insurance, tolerability, and goals.
If you're weighing these options, the most useful next step is a conversation with a prescribing clinician — and a closer look at the peptides on the horizon. Continue with our complete BPC-157 guide [INTERNAL LINK: BPC-157 guide — Post 3], the deep dive on retatrutide [INTERNAL LINK: Retatrutide guide — Post 5], and the practical guide to peptide therapy access in 2026 [INTERNAL LINK: How to get peptide therapy — Post 10].